Medina ER says it is committed to high-quality care ‘as quickly as possible’
Quick Questions with Dr. Richard Elman and Mackenzie Smith

Photos by Tom Rivers: Dr. Richard Elman serves as medical director of the Emergency Room at Medina Memorial Hospital. He is pictured with, from left: Amanda Luckman, secretary of the ER (sitting); MacKenzie Smith, nurse manager and stroke coordinator (in back); and Maria Piotrowski, a registered nurse.
MEDINA – Some of the new faces at Medina Memorial Hospital’s Emergency Room may look familiar to community members.
Dr. Richard Elman is the ER’s medical director. He worked for the hospital in the 1990s. He returned when the hospital in August partnered with TeamHealth, a physician services organization, to provide staffing for the ER, which serves about 10,000 patients annually.
TeamHealth started work in the Medina ER on Aug. 1. It has five full-time staff and six part-timers working at Medina. That includes physicians, nurse practitioners and physician assistants. TeamHealth works with about 3,000 hospitals in the country.
The ER’s nursing staff is also managed by MacKenzie Smith. She grew up in Medina and was working at a large hospital in Rochester before returning to work in her hometown about 1 ½ years ago. Smith also is coordinator of the designated stroke center at the hospital.
Smith said the ER has been focused on improving care and providing it “as quickly as possible.”
She is pleased with that push for excellence. The ER also has updated equipment with computers mounted in the two trauma rooms, new nurses’ stations and cabinetry. Wireless scanners and redone floors are coming to the ER, which includes seven rooms, plus a triage room.
The two ER leaders were interviewed last week at the hospital.
Question for Dr. Elman: Why do you think so many hospitals are contracting with TeamHealth for ER services, rather than trying to do their own staffing?
Answer: There is a lot you can do when you are that large. They are a very well-oiled organization. They provide a lot of resources and support to all of their members. There is continuous education, best practices – how should this ER be running and what can we do more efficiently – that is offered to us and there are expectations that we implement these processes as we move forward.
Question: Have you already identified processes that could be improved in Medina?
Answer (Dr. Elman) : Oh we’ve already started making some changes since we’ve been here.
Answer (Smith) : Dr. Elman is also the chairman of emergency medicine for Catholic Health Services.
Answer (Dr. Elman) : I spent the last 13 years as chairman and facility medical director for South Buffalo Mercy Hospital. Over the last year and half I’ve been chairman of the Department of Emergency Medicine for the Catholic Health System. (Medina and the Catholic Health System have an affiliation.)
Question: What are some of the things that are improved at the Medina ER?
Answer (Smith) : It’s fair to say things are improved. Dr. Elman is working on new policies and really bringing us up to speed for a lot of evidence-based practice and to provide the best care and treatment for our patients.
Answer (Dr. Elman) : I work about 10 shifts a month here on average so I’m actively involved not just in the administrative aspect but the clinical aspect. So I walk the walk. I work here and see what issues there are and what we can do to improve it. I work collaboratively with MacKenzie and the team we have down here – nurses, aides, PAs and our docs – to communicate the messages we need to get through, about how we want to change what we’re doing.
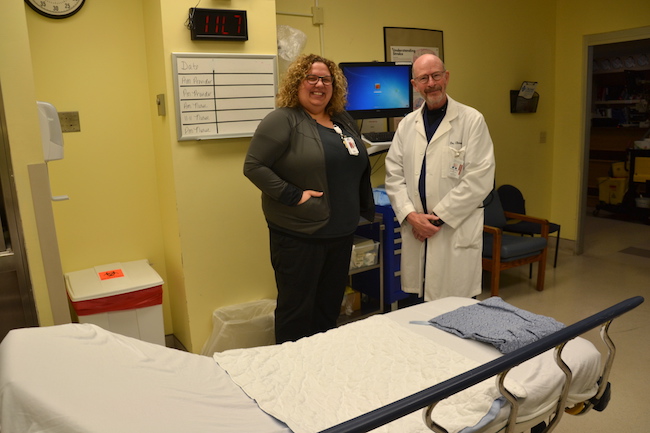
MacKenzie Smith and Dr. Richard Elman are pictured in one of the trauma rooms with a new mounted computer, which makes it quicker to enter and check medical data.
Question: If there is down time what does a doctor do here?
Answer (Dr. Elman) : I’m doing paperwork, or the schedule, chart review or working on policies. I do a lot of my administrative work in the down time.
Answer (Smith) : I do want to point out is that even though they are a national organization, TeamHealth is very involved with each individual hospital. The regional medical director is coming down in November for an EMS education night over at Medina Fire Department. They are very forthcoming with doing education.
Question: What do you think the community should know about the ER?
Answer (Dr. Elman) : We are focused on efficient quality care, reducing or improving turnaround times so patients aren’t spending hours in the ER when they don’t need to be here, to instilling best practices in medicine and in patient health.
Question: Are there statistics on that?
Answer: We’re in the process of bringing in a new electronic medical record. Once that process is completed we’ll have the ability to run reports. We look at door-to-provider time. That national goal is 30 minutes for the patient to see a provider within 30 minutes of arrival. We look at turnaround times for discharged patients, and percentage of patients who leave without being treated or against medical advice. There are national statistics or thresholds, and our goal is to be under them. Those will all be focuses of what we do.
Question: Does Medina have to submit an annual report?
Answer (Smith) : It’s a running report more for our measures of patient care and delivery, for chest-pain patients, for stroke patients, those are the metrics that we have to submit and are held accountable for. The turnaround time and the door-to-provider time is ongoing. There are some variances for that. There is some wiggle room. If your volume is very high or if your acuity is very high that makes up for the times that you are not.
Really the metrics that are reportable would be the stroke and chest pain, and the very patient-centered metrics. We are a stroke center so we have rigorous metrics we have to do for that.
We are very efficient at knowing what can be treated here and what we have to ship out. A lot of times we do have to ship out to the higher level of care facilities. But we are very efficient with our times for that. We also have a very close collaboration with Medina Fire in getting our patients out. They have a very quick time for getting patients out of here for transfers. It’s not always a common thing at other facilities. We’re fortunate to have Medina Fire.
Question: Do you have a sense of what percentage you’re able to handle here without sending to ECMC or another larger hospital?
Answer (Smith) : It all depends on what the patient is presenting for. If it’s a trauma patient they really need to go to a trauma center. Our job is to stabilize those critical patients. And that’s what we need to be excellent in: stabilization. Knowing when to get them out, we do that very quickly and efficiently.
Answer (Dr. Elman) : We can primary care. We don’t have a lot of specialists. Anybody with a complicated medical problem – a heart attack or a stroke or a trauma, or a lot of patients may be getting medical care at other tertiary care centers in Buffalo or Rochester – those patients we will probably have to transport. It’s what is best for the patient in each case.
Dr. Richard Elman enters data into the computer in the Emergency Room at Medina Memorial Hospital.
Question: If there was no ER in Medina, what would happen for the community?
Answer (Dr. Elman) : They would have to go to Batavia, Lockport, Rochester or Buffalo on their own. We can treat a fair amount here and we can stabilize what we can’t treat.
Answer (Smith) : It would be detrimental for our community. Our ER is vital for the community. It is vital for businesses coming to the community.
If you are having a cardiac arrest or if you’re loved one is having a cardiac arrest or respirator distress, it’s a very long ride to the city.
Question: How many stroke patients do you have a year?
Answer (Smith) : Last year we were between 60 and 75.
Question: Do they then go by Mercy Flight after getting the clot-busting drugs?
Answer (Dr. Elman) : It depends on their condition and whether Mercy Flight is flying based on the weather outside.
Answer (Smith) : If not they would go by Medina Fire and that’s why I say our collaboration with Medina Fire is very important. We have a very close working relationship.